Physician Blog by Edward J. Bieber, MD
Shoulder Pain – Biceps Tendonitis
The biceps tendon is a common, though often overlooked, source of shoulder pain. Most people assume that they have arthritis or rotator cuff pathology when the biceps can be the primary source of pain. It is, however, often associated with the other reasons for shoulder pain such as rotator cuff tendonitis or tearing, arthritis, impingement or instability which is why the diagnosis is not made as easily. The primary symptom is pain in the front of the shoulder and radiating down the upper arm and associated with certain motions which is very similar to the pain associated with rotator cuff pathology.
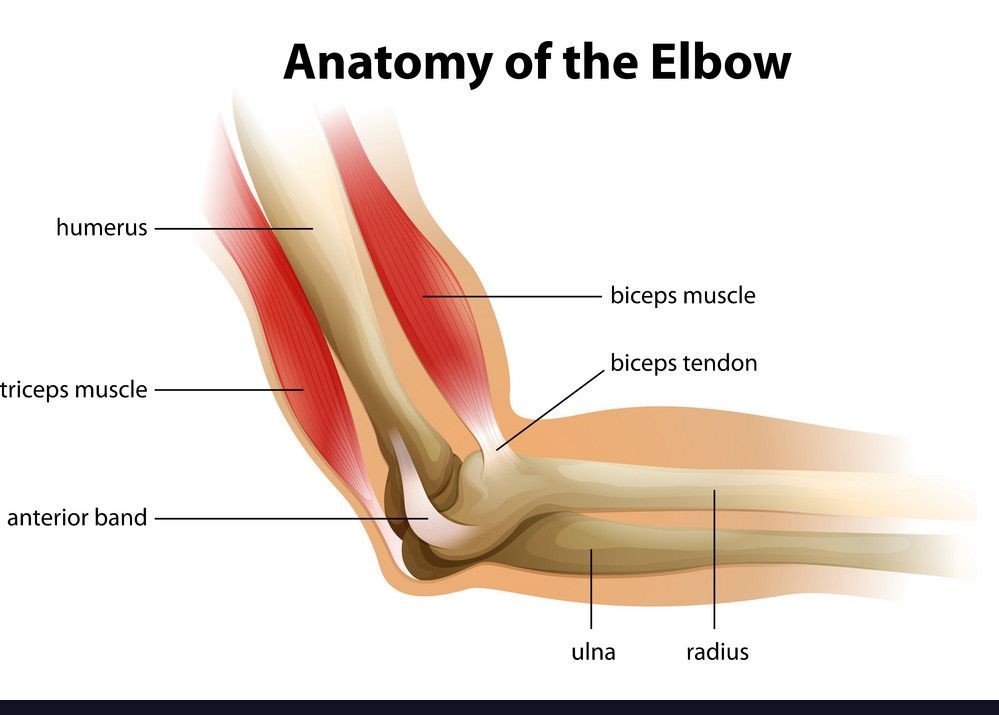
The biceps anatomy is unusual in that the muscle has tendons at both ends of attachment. It has a single tendon in the elbow and two tendons (short and long head) in the shoulder region. The short head attaches to the coracoid process of the scapula (wing bone) and is rarely a source of pathology. The long head attaches at the top of the glenoid (shoulder socket) to the labrum and then runs between two of the rotator cuff tendons and then through the bicipital groove (a narrow tunnel) on the side of the humerus (upper arm bone). The damage to the long head can occur within the shoulder joint or within the bicipital groove. There can be mechanical irritation, degenerative wear, inflammation (tendonitis) or actual tearing of the tendon (traumatic or degenerative).
The diagnosis is primary a clinical one and is made by physical exam. There is tenderness over the bicipital groove which is worsened when the shoulder internally rotates (palm down) about 10 degrees. The pain can be elicited by elevating the shoulder against resistance with the elbow extended and the forearm supinated (palm up). Pain may also be elicited by actively supinating against resistance with the elbow flexed. Although ultrasound and MRI scans may show some thickening of the tendons, they are often not reliably diagnostic.
There are a variety of treatments available. The most basic factor is that when a tendon is inflamed it must be rested because without that, no other treatments will be effective. Treatments to reduce the inflammation include NSAIDs (non-steroidal anti-inflammatory drugs such as Advil or Aleve) or corticosteroid injections directly into the bicipital groove. Once the inflammation is reduced, a careful physical therapy program can be designed to try to prevent recurrence. There are surgical options for tendonitis that cannot be controlled by other treatments or keeps recurring. These are tenotomy (cutting the long head) or tenodesis (cutting the long head and reattaching it to the humerus). There are pros and cons for both treatments but in the long run, there is no difference in strength recovery between the two techniques.
For more information or treatment, please make an appointment.
– Edward Bieber, M.D.
Dr. Edward Bieber of OrthoBethesda is the area’s most experienced total shoulder surgeon.
He has been performing anatomic total shoulders since 1986 and reverse total shoulders since 2007. He employs an integrated program of state of the art surgery with the OrthoBethesda physical therapy team to achieve superior results with both types of shoulder replacements. He has extensive experience with computer assisted directional devices and custom made devices for patients with significant bone deformity. Read more here and make an appointment with Dr. Bieber today.

Related Content
- Golfer’s Elbow: What Is Is and How You Can Heal It
- What’s the Difference Between Golfers Elbow and Tennis Elbow
- 7 Tennis Elbow Exercises to Treat Your Pain at Home
- How Long It Takes for Tennis Elbow to Heal
- Top Exercises to Avoid If You Have Tennis Elbow
- Exercises You Can Do for Tennis Elbow
- Tenodesis vs. Tenotomy
- Everything to Know About Tommy John Surgery